




 1800 278 462
1800 278 462Key Updates to AAH Released by The National Asthma Council
The National Asthma Council of Australia (NAC) has released significant updates to the Australian Asthma Handbook (AAH),1 bringing Australian asthma management guidelines into closer alignment with international best practice recommendations including those published by GINA (Global Initiative for Asthma).2
“The major change: as-needed short-acting beta₂ agonist (SABA) alone is now considered inadequate treatment for asthma in adults and adolescents.”
What’s Changed: Core Treatment Recommendations
1. New! First-line treatment recommendation: anti-inflammatory reliever (AIR) therapy
- Following asthma diagnosis, it is recommended that adults and adolescents with mild disease start treatment with low-dose budesonide-formoterol taken as needed when symptoms occur (anti-inflammatory reliever (AIR) therapy)
- Replaces traditional SABA (salbutamol) as first-line relief medication.
- Only formoterol-containing combinations are approved for this indication, as formoterol works as quickly and effectively as salbutamol (3-5 minutes) with longer duration of action.




2. Critical change: End of SABA-only treatment
- No adult or adolescent (12+) with confirmed asthma should use SABA alone.
- Even perceived mild asthma with infrequent symptoms is associated with risk of severe flare-ups and death.
- Reminder that SABA overuse is an independent risk factor for severe exacerbations.4
- SABA overuse (3+ canisters/year) significantly increases exacerbation risk.
- Using 12+ SABA canisters annually increases death risk 32-fold.
3. Stepped care approach is updated
- Start newly diagnosed patients on low-dose budesonide-formoterol as needed.
- Don’t delay starting MART (Maintenance and Reliever Therapy).For patients with significant symptoms most days a week, or frequent exacerbations, progress to ICS-formoterol MART.
- Combination devices are recommended: use of AIR or MART over single medicine devices improves adherence to the correct regimen and has a lower environmental cost.
- Step up or down budesonide-formoterol dose and frequency based on level of control.
Some patients still prefer and benefit from other ICS and ICS/LABA devices. In these cases, the role and recommendation of SABA as the reliever remains and is described in an alternative pathway in the updated AAH.
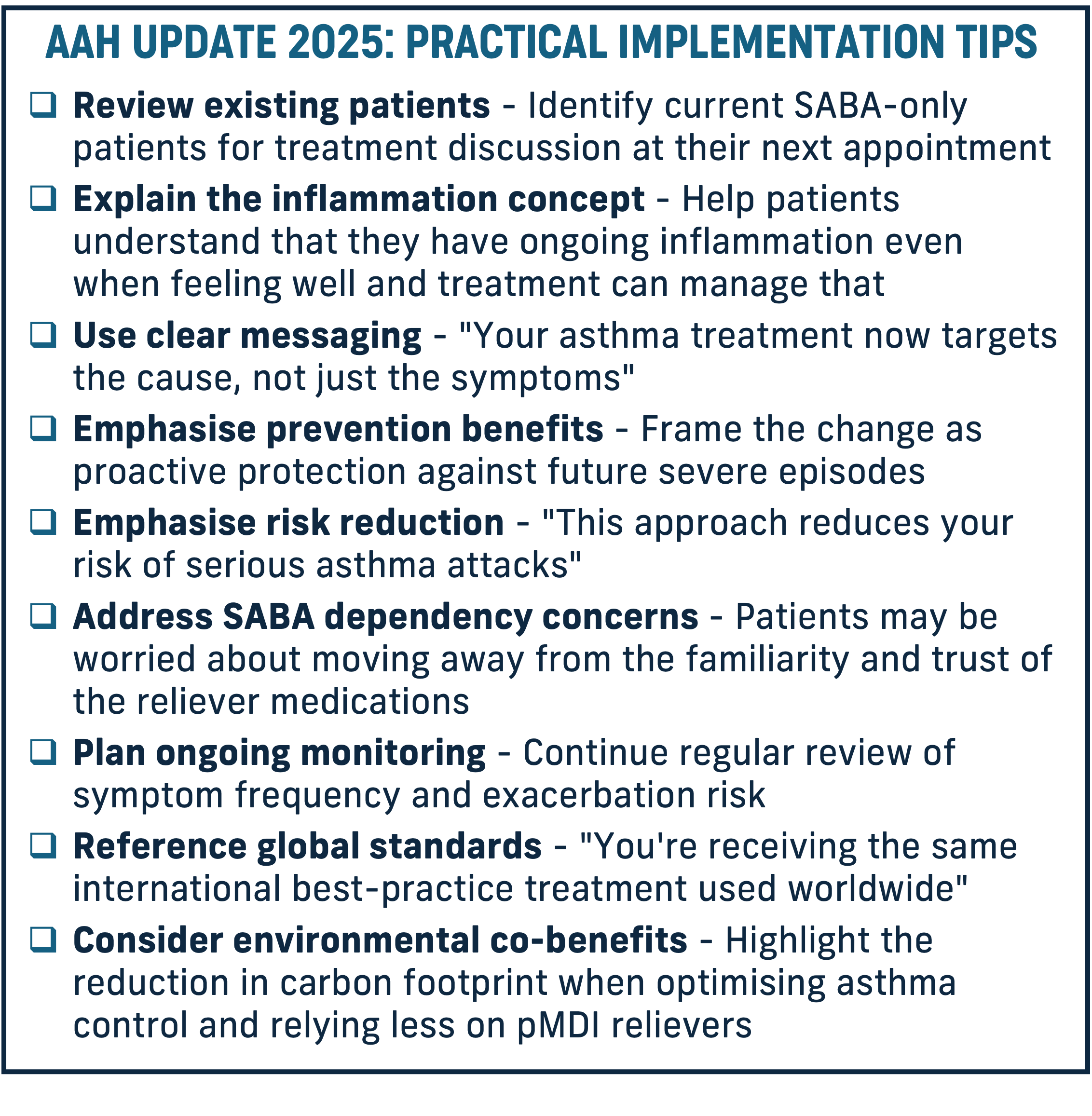
Clinical Rationale: Why This Change Matters
The updated guidelines reflect the fundamental shift in asthma management philosophy which was led by GINA in 2019.5 Asthma is a chronic inflammatory condition; educating patients that they have it all the time, not just during attacks, will be important to help them understand the rationale for treatment that targets this inflammation, rather than masking them by simply treating symptoms. This approach places primary focus on preventing severe exacerbations that lead to hospitalisation, ED visits, or death, while also rapidly treating symptoms. AIR therapy (low-dose budesonide-formoterol taken as needed) has been shown to reduce the risk of severe exacerbations requiring oral corticosteroids by 55%, compared with SABA as needed.6 With 15 million SABA inhalers dispensed in Australia each year (including those for asthma and COPD ), that’s more than 4 for each person which puts each of them at an increased risk of exacerbations.7
We recognise that these evidence-based guidelines reflect recommendations in best practice globally. The application of these recommendations in practice has potential to substantially shift the dial for people with asthma, away from flare-ups and symptom burden and towards health and quality of life. Asthma Australia sees the update to the AAH as an opportunity to refresh knowledge of the resources, treatments and solutions available to healthcare providers and people with asthma. And we continue to call for personalising asthma care according to the clinical presentation, co-morbidities and risk factors, patient preferences and behaviours, accessibility and cost issues which affect the patient. The best treatment is the one that has been decided through shared decision making as this enhances patient satisfaction and ultimately outcomes.
Resources
Patient Education
- Share or direct patients to our pages on the AAH update and other resources.
Professional Development
- Watch for upcoming educational webinars on practical implementation
- Access the full updated and interactive Australian Asthma Handbook from NAC
- Refer your patients for support beyond your consultation
- Stay updated: Subscribe to Asthma Link healthcare professional newsletter for ongoing clinical updates and practical implementation resources.
- Need guidance on implementation? Our clinical team are available to support you in understanding and implementing these important changes. Contact our Asthma Educators: 1800 ASTHMA (1800 278 462)
References
- National Asthma Council. Australian Asthma Handbook. 2025. Available at https://www.asthmahandbook.org.au/
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025. Updated May 2025. Available from: www.ginasthma.org
- PBS Medicine Listing. Department of health, Disability and Aging, Australian Government. https://www.pbs.gov.au/browse/medicine-listing Accessed 2 September 2025.
- Nwaru BI, et al. Overuse of short-acting β2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA
- programme. Eur Respir J. 2020 Apr 16;55(4):1901872. DOI: 10.1183/13993003.01872-2019
- Reddel HK, et al. GINA 2019: a fundamental change in asthma management: Treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. Eur Respir J. 2019 Jun 27;53(6):1901046. DOI: 10.1183/13993003.01046-2019
- Crossingham I, et al. Combination fixed‐dose beta agonist and steroid inhaler as required for adults or children with mild asthma. Cochrane Database of Systematic Reviews 2021, Issue 5. Art. No.: CD013518. https://doi.org/10.1002/14651858.CD013518.pub2
- Industry data supplied, September 2024.
Asthma Australia supports these evidence-based changes that bring Australian asthma management into alignment with international best practice, giving people with asthma the best chance at optimal outcomes.
Publication date: September 2025
Author: Asthma Australia